Case Study: 48-Year-Old Male with Shoulder Pain
Clinical Presentation
A 48-year-old male construction worker presented with persistent right shoulder pain and weakness, notably aggravated by overhead lifting and repetitive manual tasks at work. He reported a gradual onset of symptoms worsening progressively over several months, interfering significantly with his occupational duties.
History
Presentation: Chronic and worsening shoulder discomfort, exacerbated by repetitive overhead activities and heavy lifting.
Occupation: Construction worker, frequently involved in manual labor and overhead lifting.
Past Medical History: No prior significant shoulder or musculoskeletal injuries reported.
Medications: None.
Lifestyle: Physically active due to occupational demands, limited recreational activities outside work.
Physical Examination
Pain localized to the superior aspect of the right shoulder.
Significant weakness observed during shoulder abduction.
Palpable irregularity noted at the site of the supraspinatus tendon.
Positive clinical tests suggestive of a rotator cuff tear, including pain and weakness on resisted abduction and external rotation.
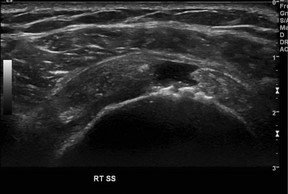
Fig. 1
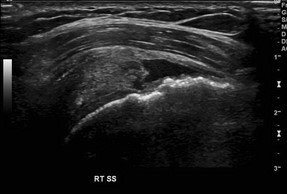
Fig. 2
Diagnostic Steps
Ultrasound Findings:
Full-thickness tear of the supraspinatus (SS) tendon, filled with anechoic fluid (thin arrows, Fig. 3). The defect extends from the bursal to the articular surface and is measured (cursors) in both the short axis (Fig. 4) and long axis (Fig. 5).
Torn, retracted tendon edges are visible, along with cortical irregularity of the greater tuberosity (thick arrow, Fig. 3).

Fig. 3

Fig. 4

Fig. 5
Differential Diagnosis
Partial-thickness rotator cuff tear
Tendinopathy
Anisotropy artifact (ultrasound beam angle causing artifactually hypoechoic appearance)
Final Diagnosis - Full-Thickness Rotator Cuff Tear
Key Teaching Points
The rotator cuff comprises four tendons: supraspinatus, infraspinatus, subscapularis, and teres minor. Approximately 95% of rotator cuff tears primarily affect the supraspinatus tendon. Tears may extend posteriorly to the infraspinatus tendon or, less commonly, anteriorly involving the biceps and subscapularis tendons.
Common etiologies include chronic or repetitive microtrauma, subacromial impingement syndrome, and tendon degeneration.
Patients typically present with shoulder pain and weakness, particularly evident during abduction.
US findings
Normal Rotator Cuff: On ultrasound, a normal supraspinatus tendon appears homogeneous, echogenic, and displays a fibrillar echopattern with consistent thickness tapering at its insertion. The tendon should be noncompressible with a smoothly convex outer contour. Short-axis (Fig. 6) and long-axis (Fig. 7) imaging demonstrate these normal features clearly. A hypoechoic area at the tendon insertion (Fig. 7) can be attributed to anisotropy and disappears when the transducer is adjusted to a perpendicular angle relative to the tendon fibers.
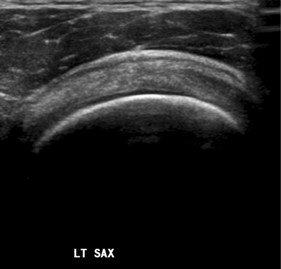
Fig. 6

Fig. 7
Full-Thickness Tear: Identified by an anechoic or hypoechoic tendon gap filled with fluid or hypertrophic synovium extending from the articular to the bursal surface. Findings may include tendon retraction, an uncovered humeral head in larger tears, sagging of echogenic peribursal fat into the tendon gap (more apparent with compression), cortical irregularity of the humeral head, and fluid within the subdeltoid bursa. Long-axis imaging (Fig. 8) may reveal loss of normal tendon convexity, retracted tendon edges, and heterogeneous material, likely representing synovial hypertrophy, within the tendon defect.

Fig. 8
Partial Tear: Characterized by a well-defined hypoechoic or anechoic defect disrupting the normal echogenic fibrillar pattern, visible consistently across multiple imaging planes. Superficial convexity of the tendon remains preserved. Partial tears may extend to the articular or, less frequently, the bursal surface, and may also present as intrasubstance or interstitial tears without surface disruption. Tendon thinning and volume loss are commonly associated findings.
Anisotropy Artifact: When the ultrasound beam is not perpendicular to the tendon fibers, it can produce artifactual hypoechoic areas, typically involving the deep surface, which shift or resolve with changes in transducer orientation.
Tendinopathy: Manifests as tendon thickening, decreased echogenicity, and heterogeneous texture without a discrete defect.
Management:
Ultrasound and MRI have comparable accuracy for diagnosing rotator cuff tears.
Surgical intervention, often arthroscopic, is considered based on tear size, retraction, patient symptoms, and functional requirements.
Occupational management involves ergonomic assessments, workplace modifications, and preventive strategies to reduce repetitive strain and reinjury.
Reference
Scoutt LM, Hamper UM, Angtuaco TL, Scoutt LM, Hamper UM, Angtuaco TL, eds. Case 144. In: Ultrasound. Oxford University Press; 2016:0. doi:10.1093/med/9780199988105.003.0144